


|
Getting your Trinity Audio player ready...
|
OWN VOICE. ~ InPerspective by Gregg Dieguez and Mary Chitty
You didn’t miss a good debate last night, but the debate missed an excellent opportunity to set things straight regarding COVID-19. I was furious with both candidates for what they did, and didn’t, say – compared to what is critical for the American public to understand. Here’s what you need to know about lingering Viral Misunderstandings…
Footnotes: to use, click the bracketed number and then click your browser Back button to return to the text where you were reading.
Images: most will enlarge for improved readability in a new window when you click on them.
Harris cited some general statistics about how poorly the U.S. has done in managing COVID, but she omitted a critical fact:
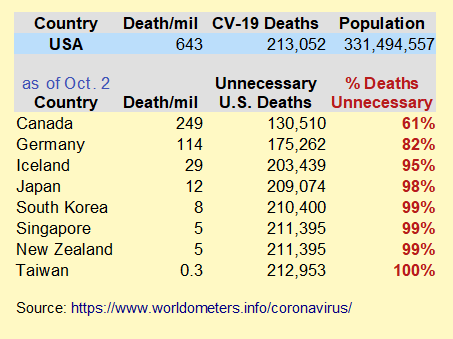
99% of the COVID deaths in the U.S. could have been prevented with competent leadership. [chart at right >] Further, she let Pence ramble on about a Vaccine – and we will need one – without pointing out that over 70 countries beat the Virus down WITHOUT a Vaccine (‘beat it down’, I said, not ‘eliminated it’. It can return.)[1]
The Vaccine effort is a distraction from both: A) what we need to be doing NOW, and B) the incompetence of a Federal Administration which: denied the seriousness of the virus, wasted time praising China until a trade deal was signed, failed to use a proven international test, and failed to secure borders (like ours with Europe, and having only porous restrictions on China) until well after it mattered. Most of what OUR Feds did was raise medical supply prices by initiating an uncoordinated inter-state bidding war, and then stealing the PPE purchased by States from them on the airport tarmac (unless the states: a) hid the shipment, and b) brought state troopers to guard the shipment), oh, and hoarding PPE in the Federal stockpile (see Kushner quotes).
Of course the Feds have funded a vaccine exorbitantly, but they want you to overlook the fact that 70 countries beat the Virus down WITHOUT a Vaccine. Result: 100-fold more U.S. deaths per person than well-managed countries who: 1) were closer “downstream” to China, and 2) didn’t have our advantages in Pandemic preparedness, but: 3) did have a Significant Advantage in Leadership. I can’t think of a more starkly obvious, and huge, failure of leadership in our nation’s history. The unnecessary wars in Iraq and Viet Nam have cost less in lives and money than our failure to contain COVID-19.
The White House has even denied allowing the CDC involvement in contract tracing for dozens of cases among our national leadership in the Capitol!
https://www.cbsnews.com/video/white-house-rejects-cdc-help-with-contact-tracing-efforts/
In contrast, here’s how good contact tracing has been done in other countries:[3]
Americans enamoured with New Zealand's handling of COVID don't even know the extent of how good it is: our most recent small cluster of cases was followed in such detailed contact tracing and gene swabbing that they traced 2 cases to a trash can lid & an elevator button.
— Carrie Rudzinski (@shutterdove) October 7, 2020
There are other ‘Viral Misunderstandings’ lingering that need to be put to bed: herd immunity, vaccines, and hydroxychloroquine. I’m tempted to call them myths, because of the exaggerated hopes placed on them by a desperate Federal government and populace, but there is a scientific basis for those ideas.
1. Herd Immunity & Vaccines:
This hope just won’t go away, but let’s be clear about how much damage has to occur to reach that level of national infection and quasi-immunity. Here’s some background paraphrased from the Lancet: History of herd immunity, Sept 19 2020. In late August, sources revealed that the White House might be pondering a policy of herd immunity. Officials issued a prompt denial. The appeal of herd immunity is easy to understand: if it is reached, the epidemic winds down through gradually decreasing levels of illness and death. Likely the illness and death such an approach would require have prompted a strong backlash. The language of herd immunity is part of the problem. A herd usually describes domesticated animals, especially livestock. Herd animals like cows, goats, or sheep are sacrificed for human consumption. Few humans want to be part of that kind of herd.
The cost in human suffering to reach herd immunity through natural infection would be very high, especially in the absence of improved patient management and without optimal shielding of individuals at risk of severe complications. COVID-19 has an estimated infection fatality ratio of 0.3–1.3%. Assuming an optimistic herd immunity threshold of 50% [67% is more likely], for countries such the USA, this would translate into 500,000–2,100,000 deaths. Those deaths would be another 33% higher with a 67% herd immunity threshold. [2]
For countries in the Northern hemisphere, the coming autumn and winter seasons will be challenging with the likely intensification of viral circulation, as has recently been observed with the return of the cold season in the Southern hemisphere. To date, only non-pharmaceutical interventions, such as social distancing, patient isolation, contact tracing, face masks and hand hygiene, have proven effective in controlling the circulation of the virus and should therefore be strictly enforced. Potential antiviral drugs that reduce viral loads and thereby decrease transmission, or therapeutics that prevent complications and deaths, may become significant for epidemic control in the coming months. This is until vaccines become available, which will allow us to reach herd immunity in the safest possible way. Let me emphasize: over 70 countries have controlled the virus with those longstanding public health measures and WITHOUT a vaccine. Herd immunity is a last resort for countries too lazy or stupid or under-equipped or undisciplined to learn from 100 years of Pandemic history. That should NOT be the U.S.
It is true that vaccines are particularly well-suited for creating herd immunity because their allocation can be specifically targeted to highly exposed populations, such as health-care workers or individuals with frequent contact with customers. Moreover, deaths can be prevented by first targeting highly vulnerable populations, although it is expected that vaccines may not be as efficacious in older people. Vaccines may thus have a significantly greater impact on reducing viral circulation than living with hundreds of thousands more deaths to attain a naturally acquired level of immunity.
So, YES, please, by all means a vaccine! – but we shouldn’t have to die while waiting for it.
Follow the basic public health measures, like most of the rest of the world, and live to celebrate the end of COVID-19. Or, deny reality and live with the consequences.
2. Hydroxychloroquine:
Nope, still not proven useful. In fact, it’s dangerous. Some recent findings:
From the NY Times Oct 5 2020: Follow-up studies found the drug neither sped recovery nor prevented healthy people from contracting the coronavirus or progressing to serious disease. The F.D.A. ultimately revoked its emergency approval. The agency now warns that hydroxychloroquine can cause dangerous abnormalities in heart rhythm in coronavirus patients, which matters a lot because CV-19 is also destroying heart muscle.
Researchers have also conducted large reviews concluding that hydroxychloroquine does not benefit Covid-19 patients, and have reaffirmed the risks of side effects in these individuals. It does work on malaria patients, trading the risk of damages from hydroxychloroquine against the greater harm from acute malaria, presumably in patients without pre-existing heart issues.
Also, from the Lancet Sept 21 2020 Hydroxychloroquine was not associated with a preventive effect against SARS-CoV-2 infection in a large group of patients with rheumatological conditions.
Those are very credible sources, so there’s no new evidence of efficacy.
THIS JUST IN:
For the first time history (over 200 years), first Scientific American, and now the New England Journal of Medicine: “Never before have the journal’s editors collectively weighed in on an election, let alone a presidential race.”
Recognition goes to Eric Rubin, Chief editor of New England Journal of Medicine and Professor @HarvardChanSPH, and the rest of the editors @NEJM for breaking with decades of precedent and taking a stand against a dangerously incompetent administration. https://t.co/Zkw7yp7SWe
— Michael Mina (@michaelmina_lab) October 8, 2020

FOOTNOTES:
[1]
FALL RESURGENCE OF COVID-19
And, in the news today, to punctuate the statement above about a fall outbreak, Europe has been surging in cases, and things have gotten worse in the U.S. as well, [chart, right>] which I attribute to attempts to reopen schools, superspreader events like the Sturgis Motorcycle Rally and Trump rallies, and states without the willpower to control the virus (as other countries have) by means of public health discipline and which allowed some reopening.
[2]
Excerpted and paraphrased from a recent article in Nature Reviews Immunology Sept 9 2020 https://www.nature.com/articles/s41577-020-00451-5
[3]
NZ Rubbish bin and elevator button
https://www.rnz.co.nz/news/national/427446/rubbish-bin-the-likely-source-of-covid-infection
More From Gregg Dieguez ~ “InPerspective”
Mr. Dieguez is a semi-successful, semi-retired MIT entrepreneur who causes occasional controversy on the Coastside, and is now a candidate for the MCC. He lives in Montara. He loves to respond to comments.  Lacking a high school diploma, Mary Chitty, hoodwinked a Yale College desperate for women into granting her a BA in Anthropology (Cum Laude). Following that she received an MSLS from the University of North Carolina Chapel Hill and rose from being a superb researcher into becoming a Biopharmaceutical librarian, taxonomist and ontologist, fact checker, scientific editor, and book reviewer. Don’t mess with her.
Lacking a high school diploma, Mary Chitty, hoodwinked a Yale College desperate for women into granting her a BA in Anthropology (Cum Laude). Following that she received an MSLS from the University of North Carolina Chapel Hill and rose from being a superb researcher into becoming a Biopharmaceutical librarian, taxonomist and ontologist, fact checker, scientific editor, and book reviewer. Don’t mess with her.



Great article, Gregg.