


|
Getting your Trinity Audio player ready...
|
OWN VOICE. ~ InPerspective by Gregg Dieguez and Bruce Laird —
“It’s quiet out there…too quiet….” You’ve heard that quote from every pinned-down cavalry man in a Western or fox-holed GI in a war movie – just before the attack.[1] And that’s what we’re hearing from the experts about COVID now, including Dr. Michael Osterholm [the director of the Center for Infectious Disease Research and Policy] – who warned us that we were in “the eye of the hurricane”.[2] Osterholm said there was reason for concern over the spread of the more contagious B.1.1.7 variant of the virus, which was first discovered in the United Kingdom and has since “wreaked havoc” on Europe.
Footnotes: to use, click the bracketed number and then click your browser Back button to return to the text where you were reading.
Images: Click to enlarge for improved readability in a new window.
But there really are TWO shoes we’re waiting to hear drop. One describes where we WERE, and the other foretells where we’re GOING. And to use one more movie analogy, we’re in The Great Race.
Where Have We Been?
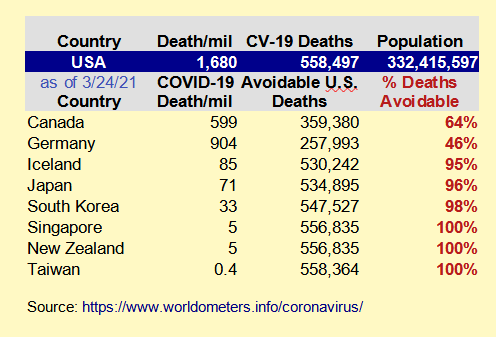
When you look at the plots of deaths and cases, it does look like we’ve been through a storm, three of them actually. But that’s not the whole story. Compare the U.S. to a country with similar economic and medical infrastructure, and we’ve done FAR worse. In fact, we were supposed to be the LEADER in infectious disease preparedness, until we were a deadly laggard. As the table below shows, almost all of our deaths could have been prevented had we reacted as Taiwan, South Korea, Iceland, New Zealand, Japan, etc. etc. did. Yes, they are more isolated geographically, but some of those countries do major business with China and SHOULD have been hit with a major first wave of infection – but they stopped it. We did not.
But the “other shoe” yet to drop here is the “excess deaths” statistic which has yet to be published for 2020. Life insurance companies have made billions in profits over the years because mortality is VERY predictable, right down to the season. But in 2020 we had a large surge in deaths, and it exceeds the reported COVID fatalities. As we know, there has been misclassification of causes of deaths in several states for political purposes: Florida, Alabama, and most recently uncovered, New York. But there’s no hiding a body bag, and sooner or later the CDC will publish the number of excess deaths – and it looks like it will be more than 100,000.[3] EDIT: It now appears this number is WAY too low, and may exceed 300,000 in excess deaths! [8]
A lot of deaths might not have been classified as COVID, but likely someone couldn’t get cancer tested because the health care system was overloaded, or a respiratory disease was worsened by the virus, and they died. So where we are is still unclear, but likely about 670,000 deaths, and counting.
There are much lower COVID death rates reported in a large number of lesser developed countries. It is often assumed that much of that is under-reporting, and that when all countries get around to tallying complete mortality for 2020 we’ll be able to assess ‘excess deaths’ everywhere, and get a more valid comparison. But there are other factors at work in COVID’s deadliness, which we’ll explain below and as explained in a New Yorker article.
Where Are We?
There are three factors frequently cited as explaining our current predicament: national leadership, public health behavior, and social vulnerability. But there may be a fourth factor affecting COVID outcomes as well: genetics. There is a Neanderthal gene carried principally by European and Asian humans which reduces the risk of severe Covid-19 infection by about 22%. It was found in all the samples researchers took of Neanderthal DNA, and in about 30% of samples from people of European and Asian origin.[4] People of purely African origin often do not carry Neanderthal DNA because they are descended from the more modern Cro Magnons whose exodus from Africa led to the demise of the Neanderthals. Thus a good part of the higher death toll in communities of color could stem from this genetic difference, and it could also be part of the explanation for lower COVID rates in Asia – along with factors such as much younger populations and more responsible public health behaviors stemming from a sense of “the interdependent self”. That sense of societal interdependency seems to have vanished from large parts of the United States, replaced with rampant individualism at any cost.
 At this moment in the U.S., with winter and holiday commingling over and vaccinations ramping up, cases in have fallen from the deadly winter 3rd surge, down to levels of the surge last summer. Though it must be noted that there is a hidden toll among those cases. About 30% of people analyzed had serious organ side effects nine (9) months after being diagnosed – lungs and brain being the most concerning. However, those studies were of patients who had been DIAGNOSED, and we’re told a lot of cases are out there which were so mild they were never diagnosed, so we won’t know the overall impact on public health for some time, until and unless waves of younger people who can’t work or play fully start showing up in doctors’ offices.
At this moment in the U.S., with winter and holiday commingling over and vaccinations ramping up, cases in have fallen from the deadly winter 3rd surge, down to levels of the surge last summer. Though it must be noted that there is a hidden toll among those cases. About 30% of people analyzed had serious organ side effects nine (9) months after being diagnosed – lungs and brain being the most concerning. However, those studies were of patients who had been DIAGNOSED, and we’re told a lot of cases are out there which were so mild they were never diagnosed, so we won’t know the overall impact on public health for some time, until and unless waves of younger people who can’t work or play fully start showing up in doctors’ offices.
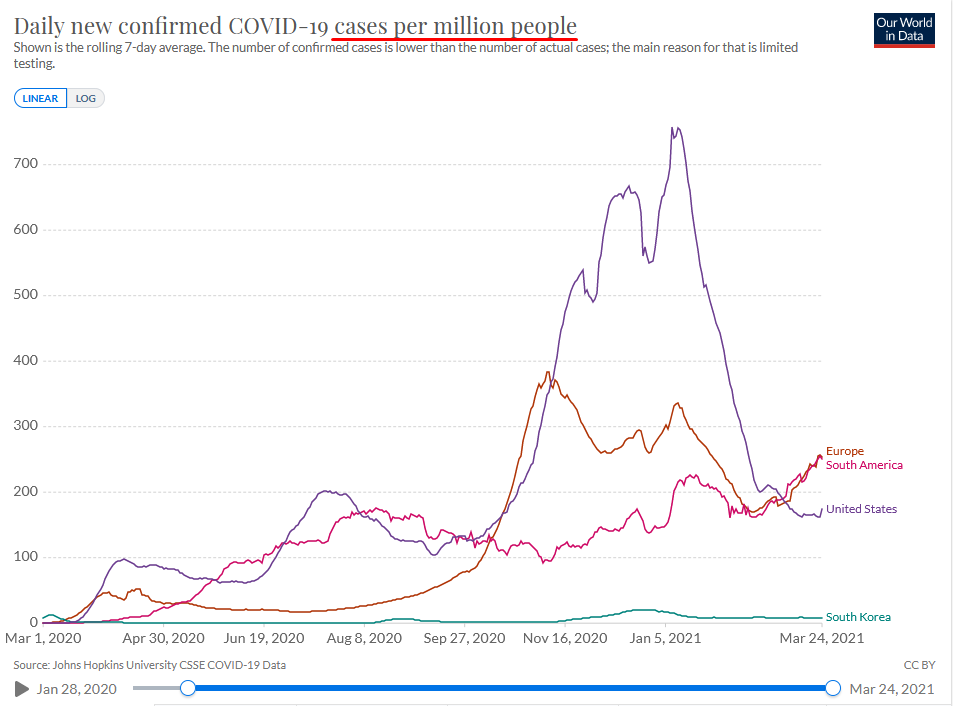
Notice something else in the chart at right: the continued rise in South America could be attributed to “their winter approaching”, but the rise in Europe? This is their summer approaching; vaccinations have started, albeit slowly. And in the U.S.? Cases have stopped dropping for weeks, and may be inching up again – in SPITE of 26% of the country having received a first vaccine dose. It’s becoming clear that variants of the virus are fighting back.
So Where Are We Going?
Which leads us to the eye of the hurricane concern. We’re now in a Great Race: the Vaccines vs. the Variants. The more people are sick, and the longer they are, the more chances the Virus has to experiment and evolve to escape our vaccines. The new variants are some combination of more transmissible and more deadly, depending on the strain.[5] And most of the current vaccine trial data was conducted BEFORE these new strains emerged, so we don’t know the degree of protection we have.
What we do know is that reinfection – either after having survived the disease or after a vaccination – is a significant possibility. We covered this concern previously, but a new study confirms it.[6] Most people who have had Covid-19 are protected from catching it again for at least six months, but elderly patients are more prone to reinfection, according to peer-reviewed research published in The Lancet medical journal last week. Prior infection gave those under the age of 65 around 80% protection against reinfection, but for people aged 65 and older it conferred only 47% protection, indicating that they are more likely to catch Covid-19 again.
The dynamics of exponential growth, which is Viral Growth, are not intuitively understood by humans. The virus takes a few weeks to gain momentum, starting small and building to a crushing crescendo. During the early days, it is not apparent whether public health measures are working or a waste of time. Here’s what we can see so far about vaccines versus the Virus and its Variants.
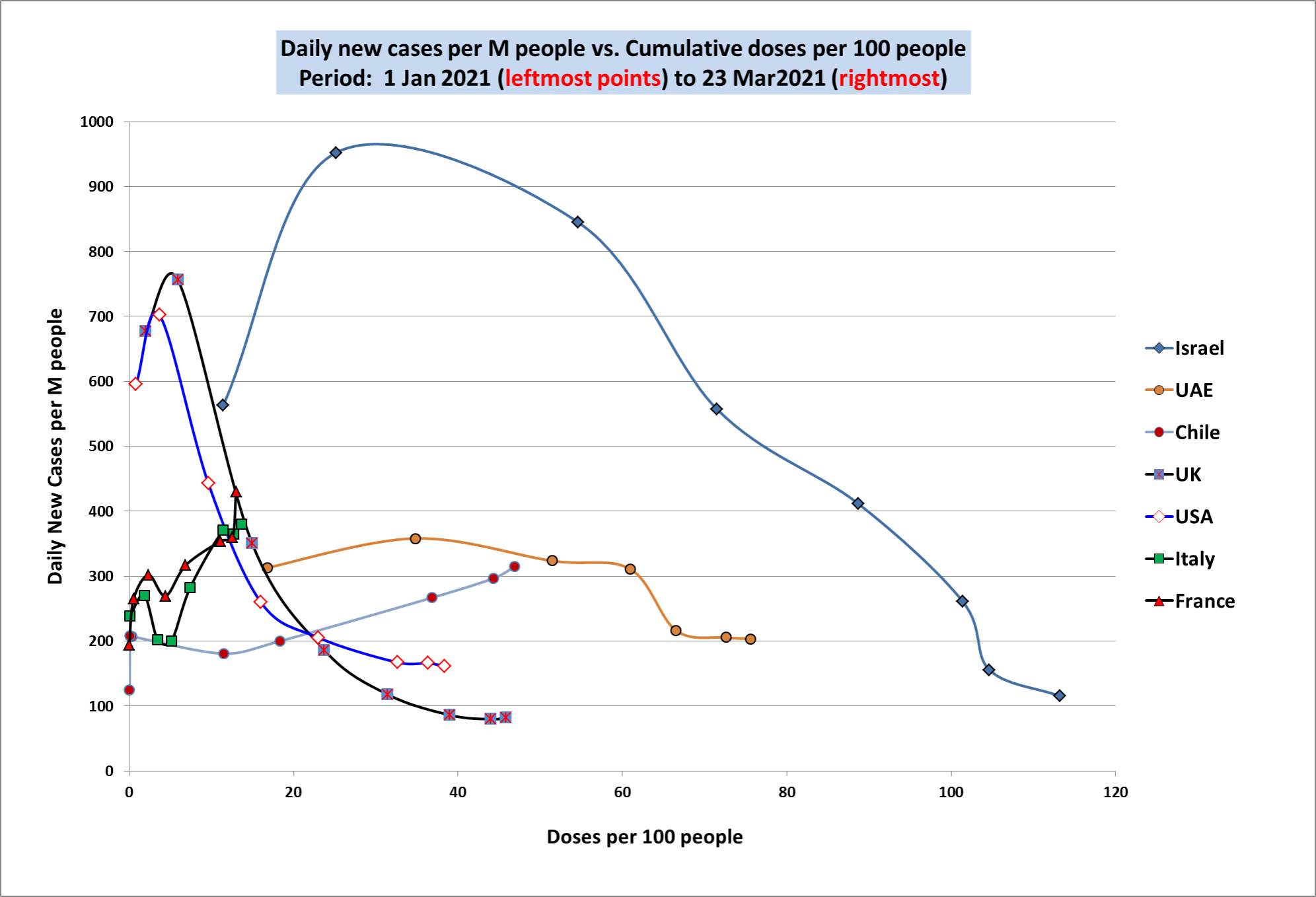
It appears that the more you vaccinate (horizontal axis), the less cases (the vertical axis) you get. [chart at right] Keep in mind some vaccines take two doses, so a country might need 200 doses per 100 people to be fully vaccinated. But look closely at Chile, Italy, and France… their cases are still going up. Further, we know the new variants are in the U.S., but we haven’t seen their full effect. And the case curves for the U.S. and U.K and Israel are not nearing Zero, they seem to be plateauing, which could reflect the re-infection problem cited above.
Below are charts for Israel and the U.S. which might make it easier to understand the interplay over time between cases and vaccination. The horizontal axis is time, and there are two vertical axes, one for cases and the other for degree of population vaccination.
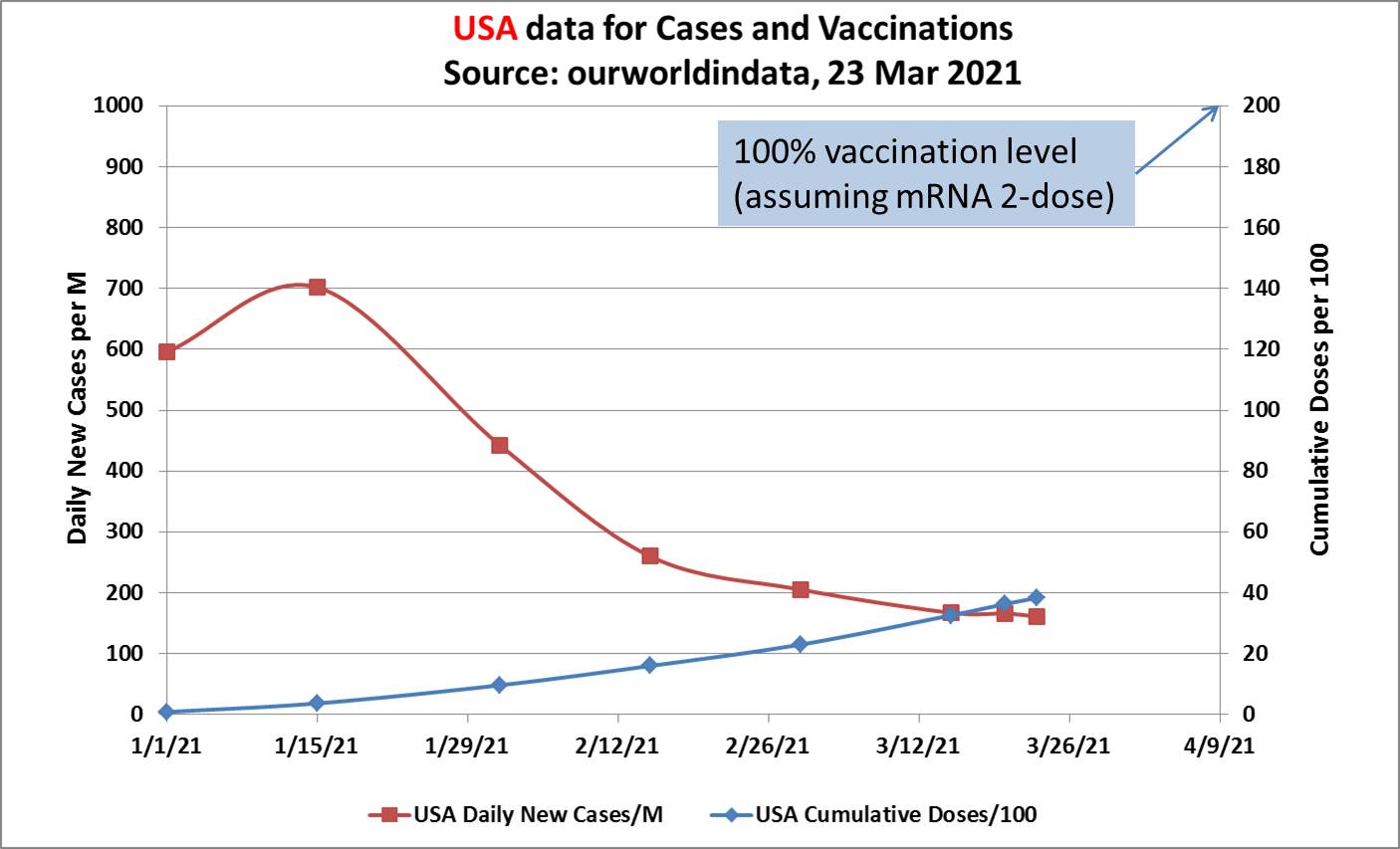
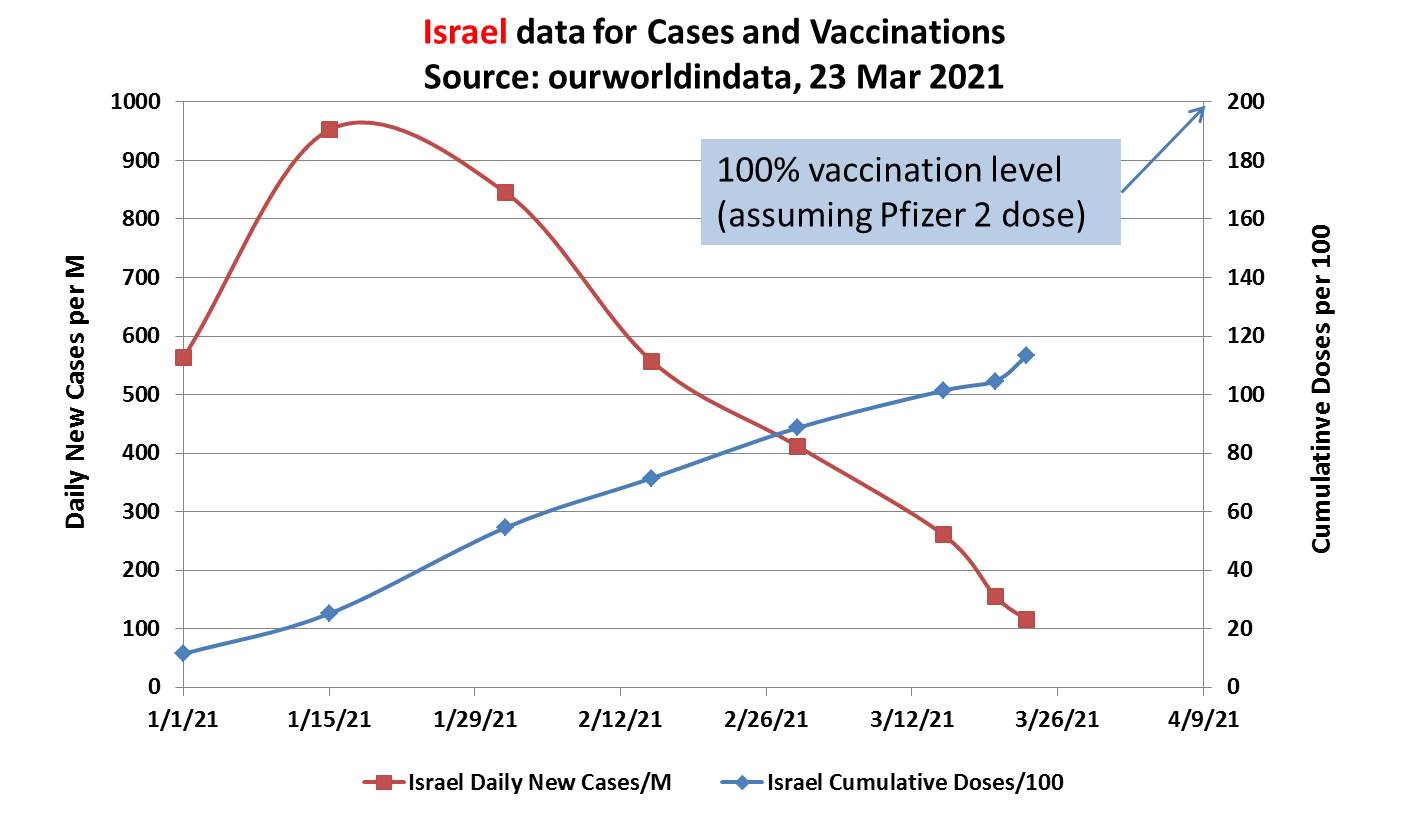
Bottom Line: These charts cannot yet prove anything. Israel aside, no country has yet vaccinated a large enough percentage of their population to significantly reduce community spread due to herd immunity effects.
Further, these charts do not show the many confounding effects from following or not following Public Health directives; the degree of business and school openings allowed; travel; etc. These confounders are almost certainly still having a bigger effect on case rates than cumulative vaccinations, even leaving variants out of it. So, we would not yet claim that the first graph shows that vaccination is winning against the variants. It’s just too early to tell, which is why experts like Michael Osterholm and Anthony Fauci are so worried about anti-Vax sentiments in the US and the EU.[7]
On top of all this, for those in San Mateo and Santa Clara County, California, your state has just decided to allocate 40% of all vaccine shipments to the most socially vulnerable zip codes, and your vaccination programs have slowed markedly. This makes plenty of sense from a harm prevention perspective, but you will have to hold your breath and wear your masks for a while longer.
And all of that is why we are concerned that we are still in the eye of the hurricane.
FOOTNOTES:
[1] Ominous Movie Line…
The earliest instance of this quote that I am aware of is The Lucky Texan (1934), a romance/western staring John Wayne, Barbara Sheldon and George ‘Gabby’ Hayes, and also in Drums Along the Mohawk from 1939. This was also popularized for newer generations in Teenage Mutant Ninja Turtles II:
Donatello: The perimeter’s quiet.
Leonardo: Yeah, a little too quiet.
In fact, there’s a recent list of 20 titles using similar phrases.
Not to mention the ever-popular: “I’ve got a REALLY bad feeling about this.” Begun in Star Wars and carried forward by Indiana Jones.

[2] Eye of the Hurricane
NEW: @Mtosterholm says “we are in the eye of the hurricane right now” on the spread of the coronavirus. #MTP
Osterholm: “It appears things are going really well, we even see blue skies … but we know what is about to come upon us is the situation with this B117 [UK] variant.” pic.twitter.com/kQbYxdL6gS
— Meet the Press (@MeetThePress) March 7, 2021
[3] CDC Excess Deaths
Currently there is a range of estimates…62951 to 161478, which averages over 110,000.
https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm
[4] Neanderthal COVID gene
https://www.pnas.org/content/118/9/e2026309118
[5] Variants Concerning
https://www.mayoclinic.org/diseases-conditions/coronavirus/expert-answers/covid-variant/faq-20505779
https://www.nytimes.com/live/2021/02/14/world/covid-19-coronavirus
[6] Reinfection with COVID-19:
News article: https://www.cnbc.com/2021/03/17/covid-reinfection-more-common-for-the-over-65s-study-finds.html
Academic study: “Assessment of protection against reinfection with SARS-CoV-2 among 4 million PCR-tested individuals in Denmark in 2020: a population-level observational study”
[7] He’s been correct before, on April 8, 2020:
In each of the eight influenza pandemics to hit the United States since 1763, a relatively mild first wave — no matter what time of year it arrived — was followed by a larger, much more lethal wave a few months later, noted Michael T. Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota. “We will go much higher in the next 12 to 18 months,” Dr. Osterholm said. Because this is a coronavirus, not influenza, it may not follow the same pattern, but it is “a much more efficient transmitter than influenza.”
[8] Updated Estimate of Excess Deaths:
From one of the three most prestigious medical journals comes this assessment:
…the reported number of COVID-19 deaths underestimates the excess deaths produced by the pandemic. Due to reporting delays and miscoding of COVID-19 deaths and an increase in non–COVID-19 deaths caused by disruptions produced by the pandemic, excess deaths are estimated to be 50% higher than publicly reported COVID-19 death counts. …COVID-19 is unlike other causes of death … because it is communicable; individuals who die from homicide or cancer do not transmit the risk of morbidity or mortality to those nearby. Every COVID-19 death signals the possibility of more deaths among close contacts.
The failure of the public and its leaders to take adequate steps to prevent viral transmission has made the nation more vulnerable, allowing COVID-19 to become the leading cause of death in the United States, particularly among those aged 35 years or older. Much of this escalation was preventable, as is true for many deaths to come. The prospect of a vaccine offers hope for 2021, but that solution will not come soon enough to avoid catastrophic increases in COVID-19–related hospitalizations and deaths. The need for the entire population to take the disease seriously—notably to wear masks and maintain social distance—could not be more urgent.

More From Gregg Dieguez ~ “InPerspective”

Mr. Dieguez is a native San Franciscan, longtime San Mateo County resident, and semi-retired entrepreneur who causes occasional controversy on the Coastside. He is a member of the MCC, but his opinions here are his own, and not those of the Council. He lives in Montara. He loves a productive dialog in search of shared understanding.
<< Mr. Laird is another semi-successful, semi-retired MIT entrepreneur but with more degrees, living in Los Altos. They roomed and caused trouble together back in the day. Bruce produces a periodic newsletter on the science and implications of COVID-19. For a free subscription, contact Bruce at: laird2007@hotmail.com



In just under a year’s time, Fauci’s messaging on reinfection and herd immunity has now mutated across dozens of variants of its own, each conveniently aligning with his political messaging of the moment. Although reinfection from new strains continues to be an avenue of research and investigation, the evidence we currently have suggests it remains uncommon. That hasn’t stopped America’s “leading infectious disease authority” from indulging in wildly irresponsible speculation from a national stage though, invariably appealing to alarmism as a pretext for continuing the same failed lockdown policies he has been peddling for over a year now.
I can understand the frustration at a year of disruption and death, but…
a) what’s Fauci got to do with it? We only mention him at the very end and he’s not the source for our research
b) what ‘failed lockdown policies’? What failed was the Not Staying Locked Down, combined with a dearth of testing resources, an almost complete absence of contact tracing, and people not obeying public health guidance. Plenty of evidence supports the efficacy of masks, for example, but lots of people refuse to wear them. The failure was actually way upstream, when we didn’t mobilize in January the way S. Korea, Japan, Taiwan, etc. did to shutdown and isolate travelers, and to test and contact trace the heck out of our own population. In fact, Iceland did a great job – without a vaccine, and without a full lockdown – they just tested the heck out of things, followed by contact tracing. https://www.coastsidebuzz.com/inperspective-sweden-done-right/
So, the lockdown was ineffective because it was too late, not adhered to, not coordinated nationally, and not accompanied by traditional public health measures a dozen other countries succeeded with.
As far as alarmism, I suggest 670,000 deaths is a real, rather than imaginary problem. And stay tuned for a fuller assessment of the long term health damage and costs. It is a real, alarming Pandemic. We’re still running about 55,000 new cases daily, and 1,000 deaths. If this were a terrorist attack or a war, it wouldn’t be viewed as “alarmism”. We could have done much better, had we decent leadership.