


|
Getting your Trinity Audio player ready...
|
OWN VOICE. ~ InPerspective by Gregg Dieguez and Bruce Laird —
We interrupt your regularly scheduled return to a life of normalcy with unfortunate but important news about the transmissibility and deadliness of the Delta variant causing COVID-19. We wouldn’t be writing this on a Sunday if it weren’t important. Below, we quickly summarize the implications before presenting Bruce’s analysis in disturbing depth.
Footnotes: to use, click the bracketed number and then click your browser Back button to return to the text where you were reading.
Images: Click to enlarge for improved readability in a new window.
First:
- If Delta catches you, you have a 5% chance of death and a 15% chance of hospitalization if you’re over 50 and UNvaccinated.
- If Delta catches you, and you are vaccinated and over 50, you have a 1.6% chance of death and a >4% chance of hospitalization.
- In Israel, about 50% of all adult cases are people previously vaccinated.[1]
- In the recent UK data (below) breakthrough (BT) infections are 26.3% of all cases; among those over 50, BT infections are 87.7% of cases.
- So, we advise against catching it, and if you’re vaccinated it appears that risk is under 1% – which is still a lot of people.
Second:
Depending on whether you get your public health news from the UK, the US, China, or Australia, you can catch Delta in…
- 3-5 seconds of exposure,[2] or
- 5-10 seconds of exposure, or
- 10-15 seconds of exposure…
- So, get the best vaccine you can, as soon as you can, and……
- Wear a facemask, because people involved in those cases of contamination via fleeting encounters were NOT doing so, and…….
- Don’t hang around with unvaccinated people.
How’s It Going?
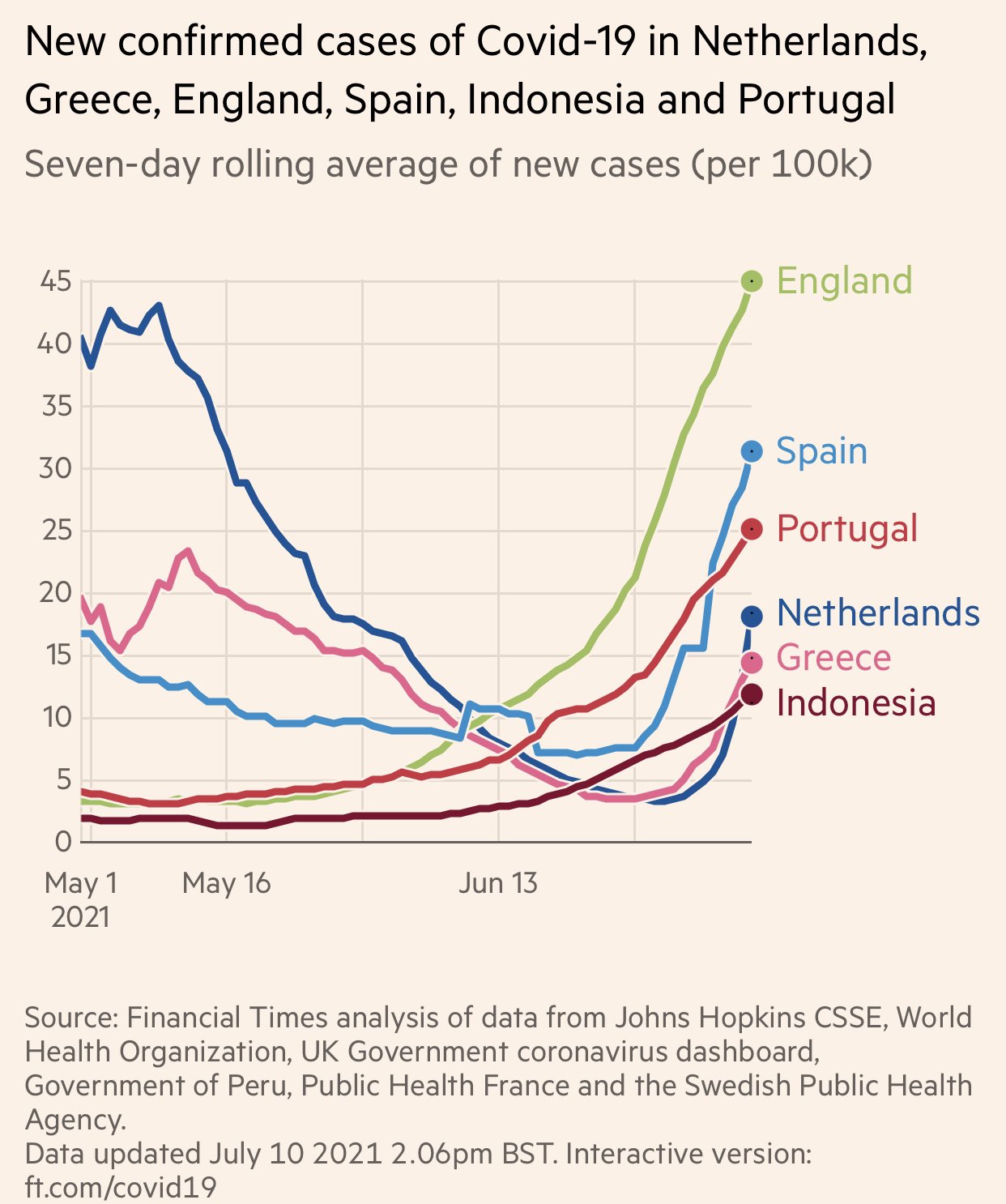
We’ve seen this before, where Europe leads the U.S in COVID catching, and here’s what’s happening now: A near-vertical surge of cases in the past few weeks. Because: Delta.[3] There have now been at LEAST 3,869 variants of SARS-C0V-2 found, and those are just the ones we found with limited genome testing. Lambda is not far behind, and other variants are in the wings – because sick people keep being breeding grounds for viral evolution.
It means about 11% of the U.S. Population could contract the Delta variant of COVID-19. Of course that outcome depends on many factors, including: people’s public health (PH) behavior, how many people survived asymptomatic cases that were never reported and thus have immunity, the rate of ongoing vaccination, and the still-to-be determined level of defense our different vaccines provide from this variant. Footnote [4] provides an explanation of how the 11% estimate was derived. We expect some correlation of case rates with the level of regional vaccine coverage, or lack thereof.
1. Changes in daily new cases vs. vaccinations for selected countries
2. Statistics for the Delta variant in the UK, through 21 Jun 2021
3. Estimated UK Delta breakthrough case rate
1. Changes in daily new cases vs. vaccinations for selected countries
This article brings up to date my two country graphs that show daily new cases per million population (DNCs/M) vs. percent of population with one or more doses of vaccine. My original intent in maintaining these graphs was to show how increasing levels of vaccination led to a drop in DNCs/M. The variability of real-world vaccine effectiveness, and especially the variations in human adherence to Public Health measures, has led to a more complicated picture. Here is the vaccination progress graph for three EU countries: Italy, France, and Sweden, along with Brazil, South Africa, and Japan. [Sources are https://ourworldindata.org/covid-cases] There is no time axis, but the period covered is from 1 Jan 2021 to 5 Jul 2021. Earlier data points are to the left, most recent points are to the right.
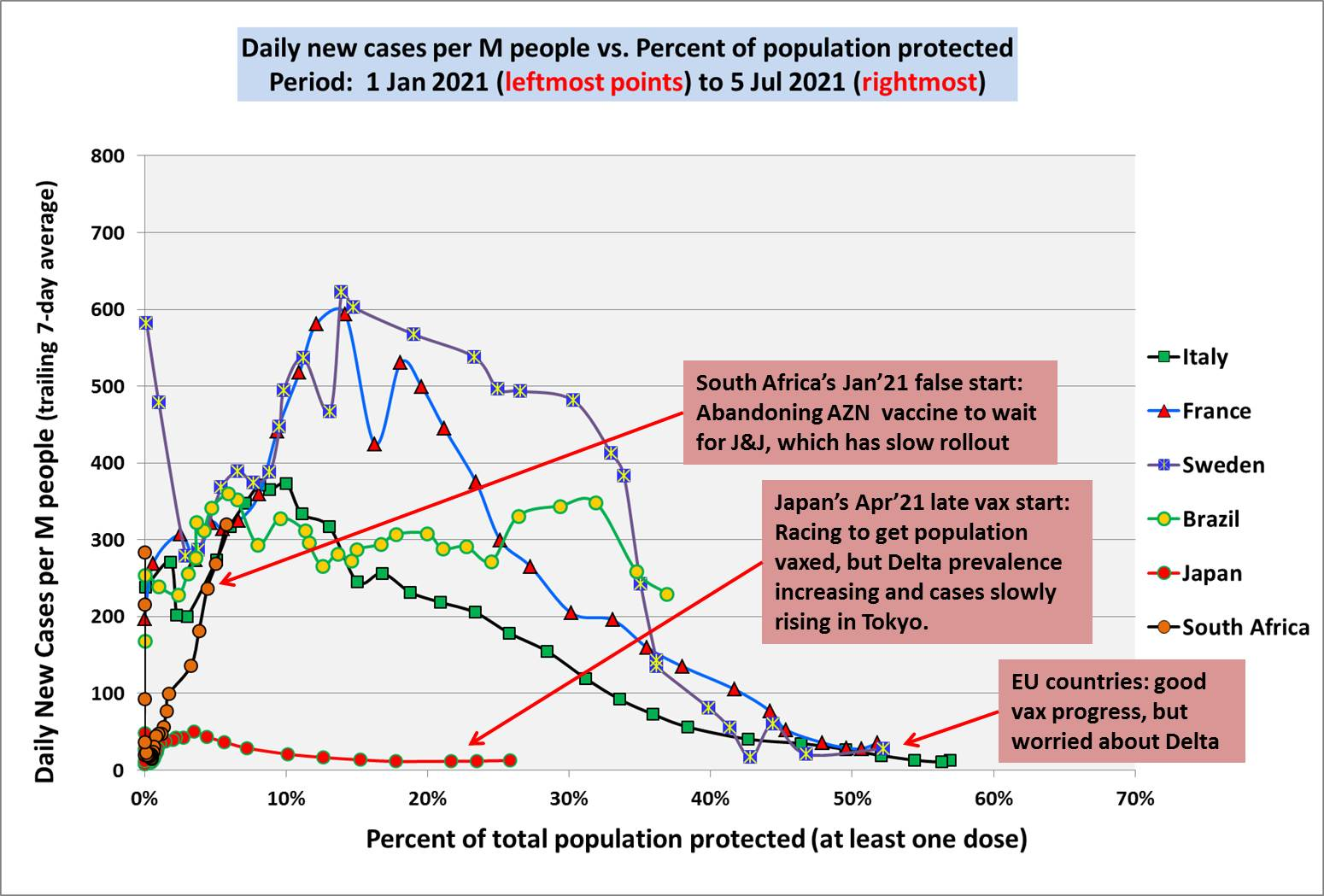
As discussed in a previous Update, the South African government made a big commitment to using the AstraZeneca (AZN) vaccine at the end of 2020, only to discover that in lab experiments, AZN showed significantly reduced efficacy against the Beta variant (B.1.351) – then the predominant variant in the country. Consequently, South Africa cancelled their commitments with AZN in January, and signed up for the J&J vaccine, which is now being administered, but only very slowly. As of 5 July, only 5.8% of the population had received at least one dose. With such a slow rollout, the country has been trying to hold down infections with PH measures. This was working to a degree, up until mid-May. But in the last month, DNCs/M have rocketed higher, from 56 at the end of May, to 320 DNCs/M on 5 July. This looks like very scary exponential growth, similar to what Michigan went through some months ago.
Sweden, Italy and France all had big spikes in cases back in Jan and Feb, but have gotten things under control with a combination of PH measures and good progress this spring with vaccinations.
I have written previously about Japan’s challenges with approving and administering vaccines. Pfizer, Moderna, and AstraZeneca vaccines are now all approved and supplies of Pfizer at least, are available in country. In fact, the Japanese government has actually overbought, and now Japan is committing to donate doses to Taiwan and other east Asian countries, even as distribution in Japan has been problematic. There are distribution bottlenecks in Japan due mainly to the fact that, by law, only doctors and registered nurses are allowed to administer the shots. This is a more serious issue in rural parts of the country, where doctors are scarce; but there are also misallocation issues. Officials in some urban areas like Greater Osaka say they don’t have enough doses, at the same time that supplies are accumulating in rural prefectures. See: “Japan’s vaccination drive slowed by distribution bottlenecks ahead of Olympics.” Japan Times, 9 Jul 2021.
Here is the picture for four countries which are vaccination leaders: Chile, Israel, the UK, and the US.
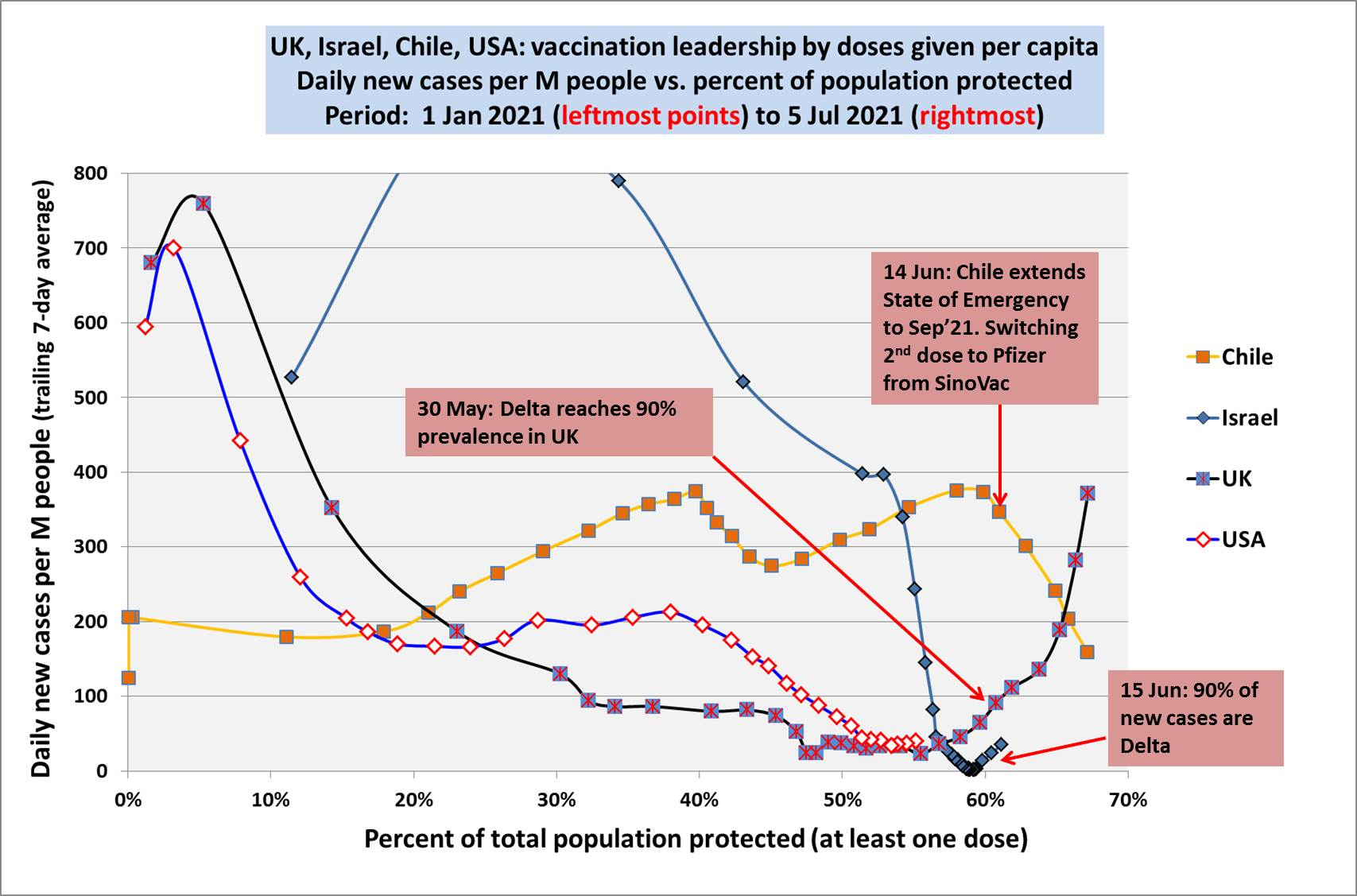
The sudden rise in cases of Delta in Israel has been pretty well documented in the public media, including some disturbing news of breakthrough cases among those fully vaccinated with the Pfizer vaccine.
I have written before about the situation in Chile, where the country started early with aggressive administration of the CoronaVac vaccine, produced by the Chinese company Sinovac Biotech. This vaccine uses a traditional inactivated virus technology, but has not demonstrated very good effectiveness in Chile. This appears to be due to a combination of two things: many people did not understand (some say the government failed to explain it well) the importance of getting both doses, so they only got one shot before relaxing their PH behaviors. Secondly, the actual field effectiveness of CoronaVac two weeks after the second dose is now reported to be only about 57%; and effectiveness after just one dose is close to zero. See: Luke Taylor, “Covid-19: Spike in cases in Chile is blamed on people mixing after first vaccine shot.” bmj, 20 Apr 2021.
From the article:
A study published by researchers at the University of Chile found that the CoronaVac vaccine was 56.5% effective in preventing infections two weeks after a second dose but only 3% effective after a single dose. Ennio Vivaldi, the university’s rector, concluded that until two weeks after the second dose is administered the vaccine “has no significant effect.” He added, “We have to be empathetic, take care of ourselves, wear masks, follow health measures, and stay home even if we have the vaccine. That’s the only way we’re going to get out of the pandemic.”
For those who read Spanish, the study referenced above is here:
“Vacunas contra el SARS-CoV2 muestran 56,5 por ciento de efectividad en la prevención de contagios.” Universidad de Chile News, 6 Apr 2021.
The upshot is that on June 14th, Chilean authorities extended the existing State of Emergency to September, 2021. Also, as the Pfizer vaccine has been available at least in limited quantities, those who did not get their second dose of CoronaVac were urged to switch to the Pfizer vaccine for the second shot.
2. Statistics for the Delta variant in the UK, through 21 Jun 2021
Public Health England publishes weekly technical briefings on the progress of SARS-2 variants in the UK, most especially the Delta variant (B.1.617.2). The latest briefing is PHE TB18, which presents cumulative data through 21 Jun 2021: “SARS-CoV-2 variants of concern and variants under investigation in England: Technical briefing 18.” 9 Jul 2021.
From the TB18 summary, principal changes and findings this week are:
● Delta variant accounted for approximately 99% of sequenced and 97% genotyped cases from 27 June to 3 July 2021
● The number of genome sequence results available is maintained but the coverage has fallen with the increasing case numbers. [My estimate: for the five months from Feb-Jun 2021, about 40% of confirmed cases were sequenced or genotyped.]
● Secondary attack rates have fallen but remain higher for Delta than for Alpha. New data is included on the prevalence of mutations of predicted antigenic significance in the global dataset – there is an increase in mutations of predicted antigenic significance over time, even outside the designated variants of concern and variants under investigation.
● Additional spike mutations are occurring on Delta but are present at relatively low frequencies both in the UK and global datasets.
● There is an increase in PCR positivity in the SIREN (national healthcare worker) cohort and a small but increasing number of possible reinfections.
● Two new variants in monitoring have been designated (B.1.619 and B.1.629).
This UK data should be of some interest both in the EU and the US, as prevalence of Delta in the UK leads these geos by around two months. In the table below, I have reproduced the data on confirmed cases, hospitalizations and deaths due to Delta, covering the period from 1 Feb 2021 to 21 Jun 2021. PHE stratifies the cases into two age groups (under 50 and 50+), and by degree of vaccination.
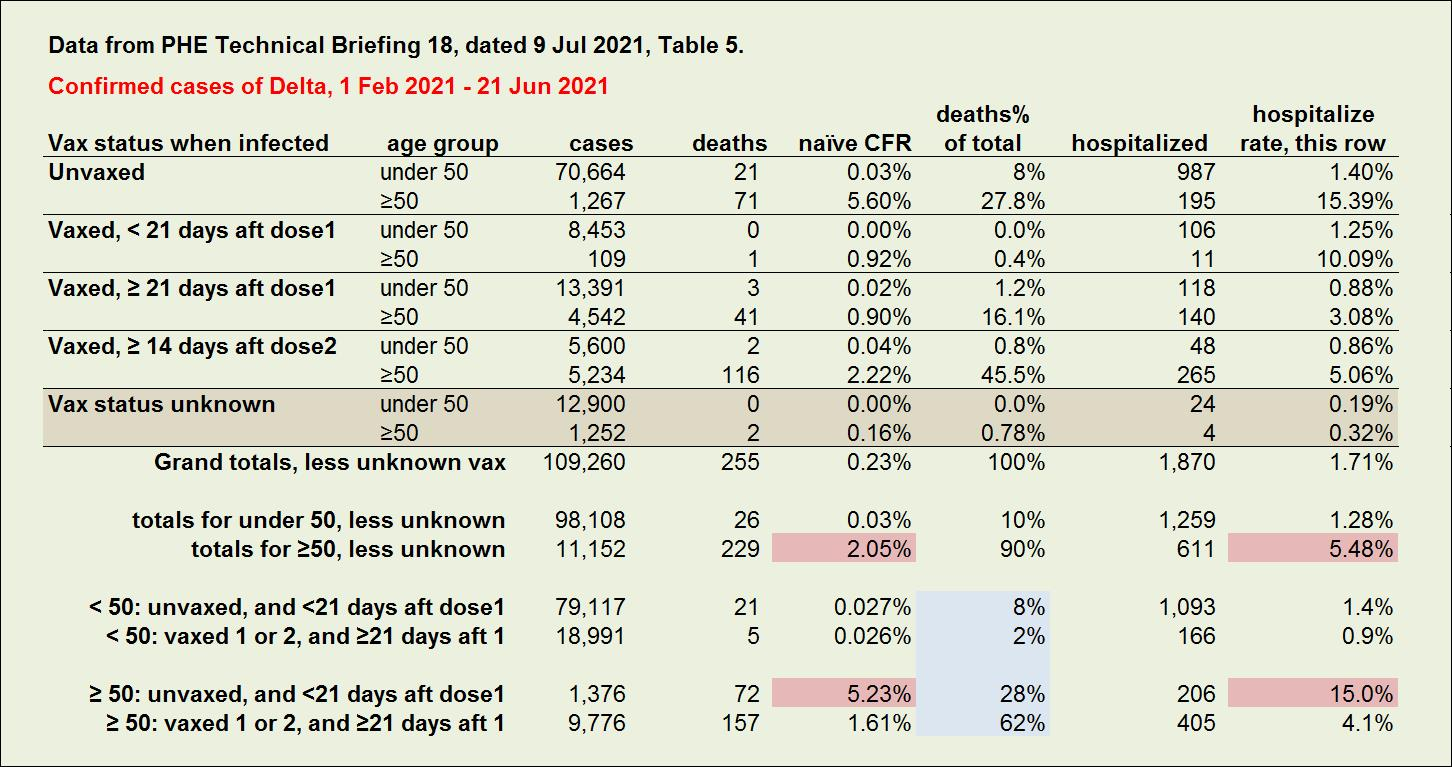
Leaving aside the 12,900 + 1,252 cases where vaccination status at the time of infection was not known, those age 50 and over have contributed just 10% of the cumulative cases (11,152/109,260), but 33% of the hospitalizations (611/1870), and 90% of the deaths (229/255). The naïve case fatality rate (nCFR = deaths/cases) for those age 50+ is 2.05%, compared to just 0.03% for those under 50. The under 50 group contributes 67% of all hospitalizations, but this is driven by the fact that the case volume is 9 times the case volume for 50+. The hospitalization rate for under 50 cases is just 1.3% (1,259/98,108 cases), compared to 5.5% for 50+ patients (611/11,152 cases).
To better see the impact of vaccinations, I’m going to combine some rows as follows:
– Count as unvaxed, those cases where infection was less than 21 days after dose 1, as well as cases having no vaccination.
– Count as vaxed those cases that were at least 21 days beyond dose 1, as well as those fully vaccinated + 14 days.
These numbers are tabulated in the bottom four rows above.
There are some differences between the vaxed and unvaxed segments in the age 50+ group. First of all, there are roughly 7 times more cases among vaxed seniors than unvaxed. This may seem a bit disturbing, as these are breakthrough cases, but we don’t know the denominator (how many total vaccinations there are, among the age 50+ population). Without knowing that number, I think this is just an indication that a very high percentage of seniors got vaccinated early.
Unvaxed seniors have a hospitalization rate of 15% (206/1376 cases), compared to 4.1% for vaxed seniors (405/9776). And the unvaxed nCFR is 5.2% (72/1376 deaths), compared to 1.6% for vaxed (157/9776). This strongly suggests that vaccination conveys some protection among seniors, from serious cases of COVID leading to hospitalization and/or death. But a naïve CFR of 1.6% among vaccinated seniors who get breakthrough cases of Delta, while it is less than a third of the unvaxed nCFR, is not exactly a great ad for the AstraZeneca vaccine (according to Scott Gottlieb, ~66% of UK vaccinations are with AZN).
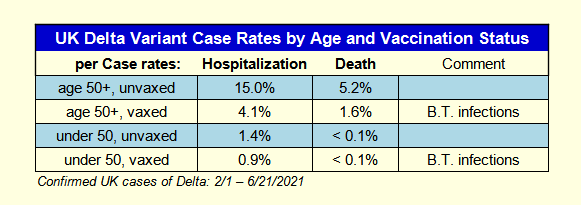
What about the under 50 cohort? In that group, there are 4.2 times more cases among unvaxed compared to vaxed, probably a reflection of lower vax rates in younger people in the general population. The unvaxed in this group have a hospitalization rate of 1.4% (1,093/79,117), compared to 0.9% for vaxed (166/18,991) – a smaller gap than for seniors. The unvaxed and vaxed nCFRs are almost identical, at 0.027% and 0.026% respectively. Again, not an especially good advert for enticing young people to get the vaccine.
We ran some statistical tests to confirm whether our findings could have been due to normal probabilistic variation. The tests confirmed with over 99% confidence that our findings are not accidental.[5].
3. Estimated UK Delta breakthrough case rate
Significant numbers of breakthrough cases are being recorded from infection by the Delta variant in the UK. Roughly twice as many breakthrough cases are recorded for those under age 50 as compared to those age 50+ (18,991 vs. 9,776), which probably says more about differences in lifestyle, exposure risks, and adherence to PH behaviors, than it does about any age dependent difference in vaccine effectiveness. Across all age groups, the Delta breakthrough cases are 26.3% of all cases where vax status is known. We can apply this fraction to the 14,152 reported cases where vax status is unknown, to estimate that there are an additional 3,726 breakthrough cases, bringing the likely total in this data to 32,493.
The Delta cases in TB18 are those that were reported through 21 June 2021. Backing off by 28 days (average of 21 and 35) takes us back to 24 May, at which point, according to ourworldindata.org, 38M people in the UK had been vaccinated with one or more doses. This suggests that, looking across all age groups, confirmed breakthrough cases of Delta are occurring in a very small fraction, 0.086% of vaccinations (32,493 cases in 38,000,000 vaccinations of one or more doses + 21 days). The actual number of breakthrough cases is higher, for at least two reasons: asymptomatic and mild cases are likely to be going untested and unreported; and only about 40% of confirmed cased in the period Feb-Jun were sequenced or genotyped. Suppose we gross up the figure of 0.086% by a factor of 1.35 for 35% of cases not reported; and by a factor of 2.5 for under sequencing. This gives a combined correction factor of 3.38, which increases my estimate for the breakthrough case rate (all ages, all degrees of severity) to about 0.3%, still a small number for those who are vaccinated.
FOOTNOTES:
[1] Israel outbreak among vaccinated::
“Children under the age of 16 — the majority of whom had not received the vaccine — were responsible for about half of the new cases, Balicer said. But about half of adults infected in the outbreak were considered fully-vaccinated — meaning that it had been at least two weeks since they received their final dose of the Pfizer shot, he said. Balicer added that the so-called breakthrough cases were expected because though Pfizer is highly effective against the virus, it’s not 100 percent protective.”
Disturbing trend in world’s most vaccinated nation:
In Israel, 5.2 million of its 9.3 million population have been fully vaccinated, however the Pfizer injection’s effectiveness has dropped to 64 per cent compared to 95.8 per cent in February. “This decline has been observed simultaneously with the spread of the Delta variant in Israel,” the Ministry of Health wrote on its website. It added the vaccine however had still averted 93 per cent of severe illnesses and hospitalisations, compared to about 99 per cent in February.
[2] Transmitted in Hallway...
We actually have CCTV footage of the encounter and it is basically a crossover of individuals. They are clearly facing each other but it is literally someone moving across from each other for a moment, close, but momentary.
[3] Current Delta trends
Explained in this twitter thread:
⚠️Bad trend—Netherlands reports a near vertical >800% increase in new #COVID19 cases in 1 week. Greece 🇬🇷 and Spain 🇪🇸 nearly matching that surge. @WHO now reports over 2 dozen countries with “near vertical” sharp rises in cases—mostly #DeltaVariant. Pandemic “Act 2” has begun.🧵 pic.twitter.com/QGM3Ta2fik
— Eric Feigl-Ding (@DrEricDing) July 10, 2021
[4] Impact of Delta on U.S.
Explained in this twitter thread:
How big of a wave of #COVID19 do we expect in the US from the Delta variant? Here I describe a simple approach to this question and attempt a rough back-of-the-envelop estimate. 1/16
— Trevor Bedford (@trvrb) June 30, 2021
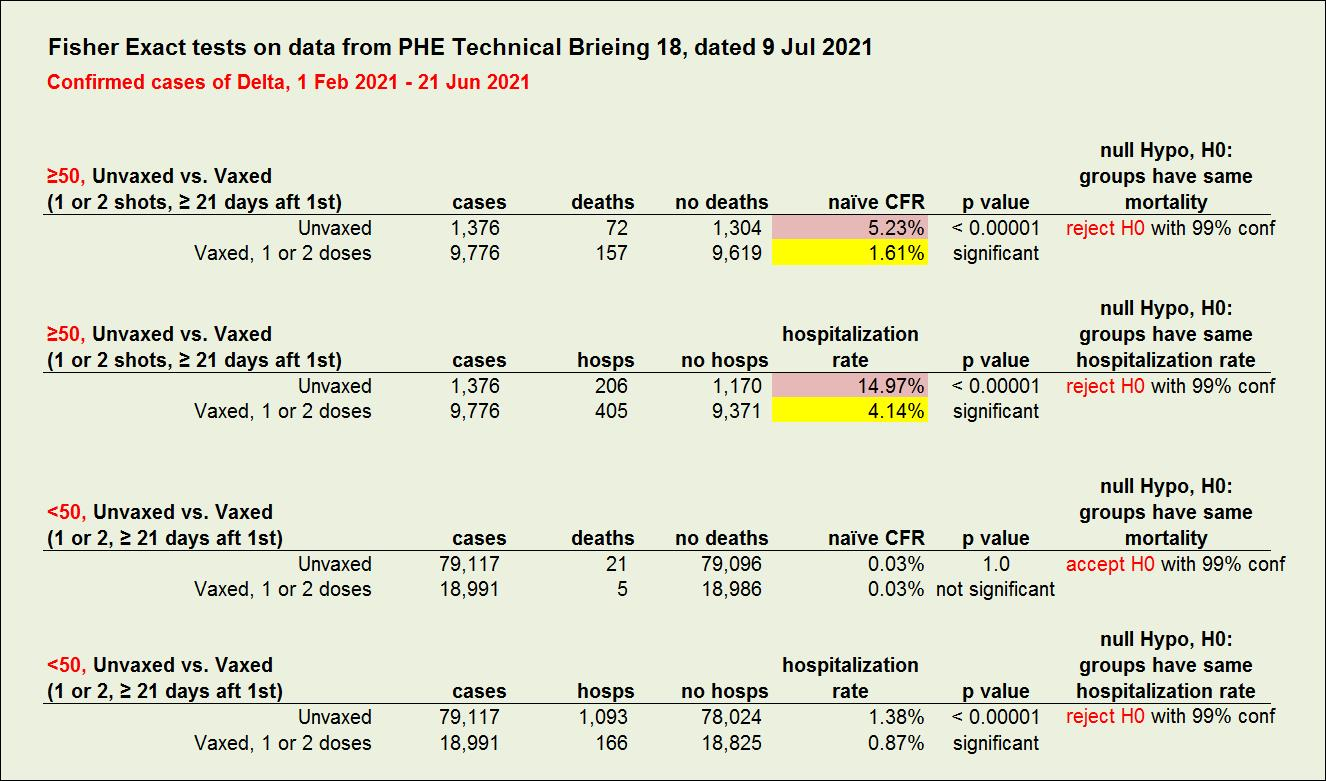
[5] Statistical Significance of our Findings:
We ran some Fisher exact tests to determine the probability of observing these numbers, given a null hypothesis that underlying rates are the same between vaxed and unvaxed. For example, in the age 50+ group, the probability of observing this number of cases and deaths among unvaxed and vaxed if they have the same mortality rate is (p < .00001), so we can say with 99% confidence that the mortality rates differ, and that those who are unvaxed are suffering higher mortality. The numbers for this test are shown in the first few rows of the table below. The results of the second test in the table yield the probability (p < .00001) that vaxed and unvaxed have the same hospitalization rate, again supporting with 99% confidence the conclusion that hospitalization rates are different, and the unvaxed hospitalization rate is meaningfully higher.
Fisher exact testing of the data for the under 50 age group indicates (p = 1) that with 99% confidence, unvaxed and vaxed people have the same mortality rates. However, the test of hospitalization rates indicates (p < .00001) that with 99% confidence, the hospitalization rates are different, with a higher rate for unvaxed.

More From Gregg Dieguez ~ “InPerspective”

Mr. Dieguez is a native San Franciscan, longtime San Mateo County resident, and semi-retired entrepreneur who causes occasional controversy on the Coastside. He is a member of the MCC, but his opinions here are his own, and not those of the Council. He lives in Montara. He loves a productive dialog in search of shared understanding. >>
<< Mr. Laird is another semi-successful, semi-retired MIT entrepreneur but with more degrees, living in Los Altos. They roomed and caused trouble together back in the day. Bruce produces a periodic newsletter on the science and implications of COVID-19. For a free subscription, contact Bruce at: laird2007@hotmail.com

