


|
Getting your Trinity Audio player ready...
|
OWN VOICE. ~ InPerspective by Gregg Dieguez and Bruce Laird, with Mary Chitty —
Why that number? Because that’s the number of COVID strains we know of since Dec. 2019 (the number changes almost daily). In here you’ll find news on: impact of the Variants you’ve never met, vaccine successes, permanent brain damage in long COVID, the new level of herd immunity, and other news you may have missed.
Footnotes: to use, click the bracketed number and then click your browser Back button to return to the text where you were reading.
Images: Click to enlarge for improved readability in a new window.
That’s correct, this virus keeps evolving, as coronaviruses have been for years. For those who never believed in evolution, where cosmic rays or other factors cause a ‘mistake’ in DNA replication and then that new organism succeeds and prospers (or not) because of the accidental change, COVID is giving us all a lesson in Warp Speed Evolution. As opposed to species with reproductive gestation times of the better part of a year, this virus is replicating uncounted of trillions of times every day, and we only hear about the ‘successes’, because someone gets ill, and tests positive for COVID, and then sometimes a gene sequence analysis is performed, and we learn we have a new ‘friend’. In the UK, they do this sequencing religiously; in the U.S., where our Public Health still lags badly compared to First World countries, not so much. But what is clear is that the virus is striving to survive.
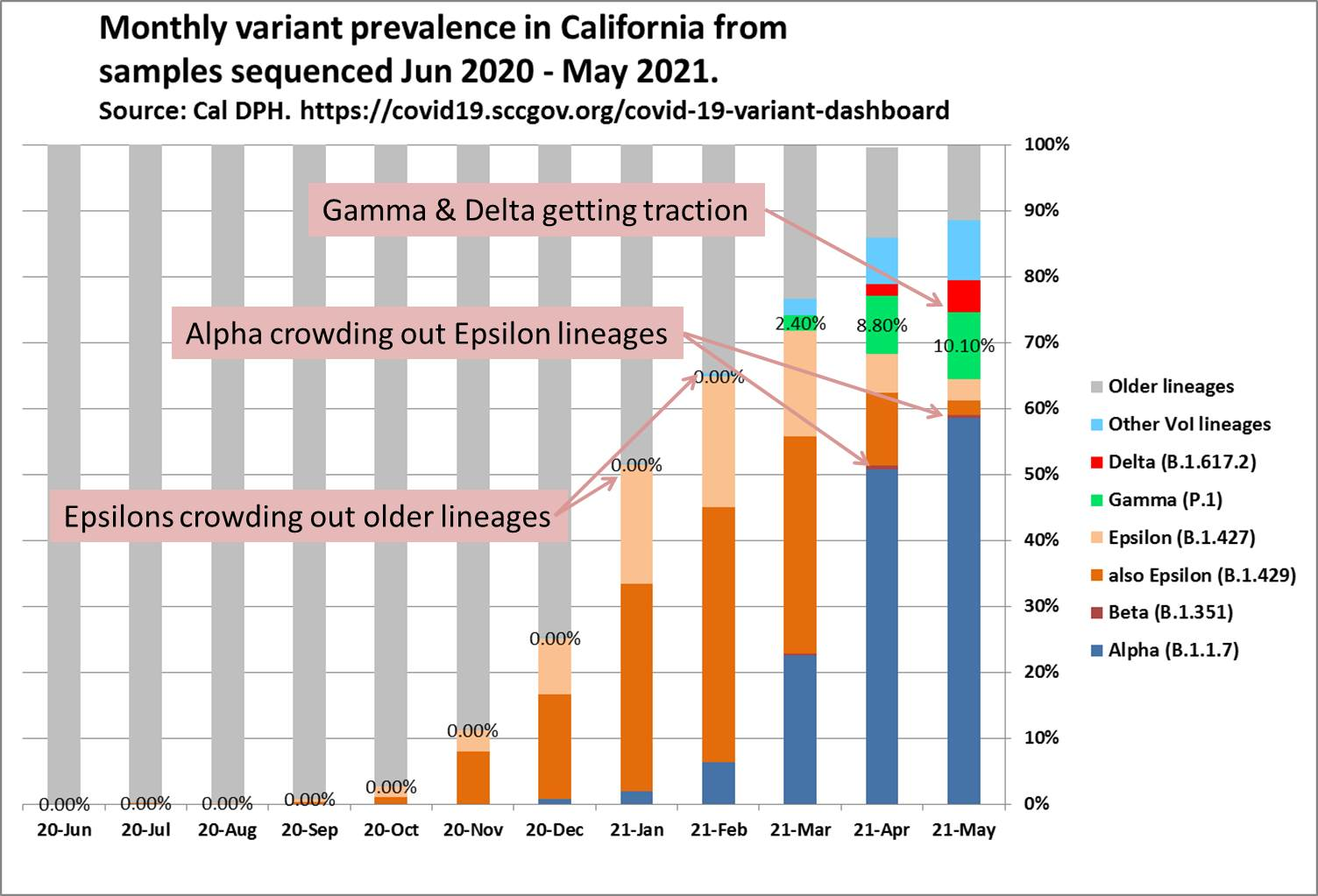
People are talking about more transmissible and deadly variants like Delta, but in the big picture that’s just another child in a long lineage. As the chart at left shows, one variant infects better and crowds out another, and it’s been going on since the Pandemic started. While the conversation today is about “Delta”, note that Gamma is now at over 10% of Calif. cases. Further, note the bright blue bar segment which contains numerous other strains, and is now over 9% of cases.[5] As long as unvaccinated people remain for the virus to experiment with, this will continue.
Pop quiz: Which of the following is most correlated with vaccination coverage in California?
(a) county death rate
(b) county percent of vote for Trump in 2020
(c) county social vulnerability index
–>Click here for answer<–
The Good News About Vaccination
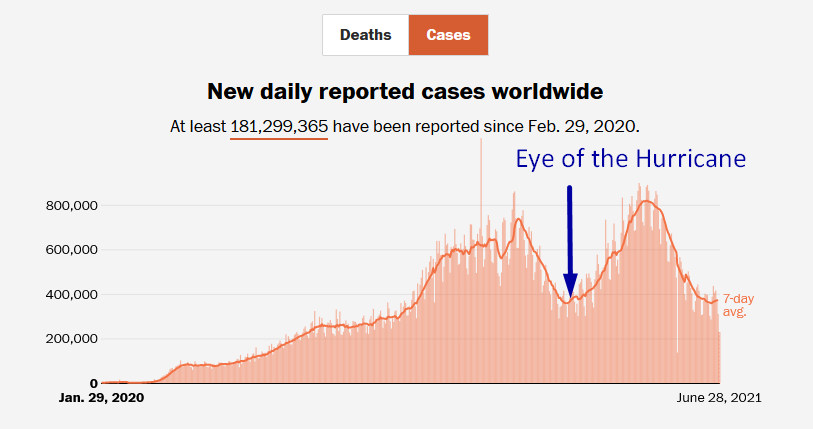
In March we were concerned about being in the Eye of the COVID Hurricane. And Globally, we were certainly correct. Even in the U.S., with an accelerating vaccination program, cases INCREASED and did not go lower for a month – either because people and elected state leadership got frustrated, or lazy, or because more transmissible variants took over. However, in countries without access to vaccines, the virus continued to surge.
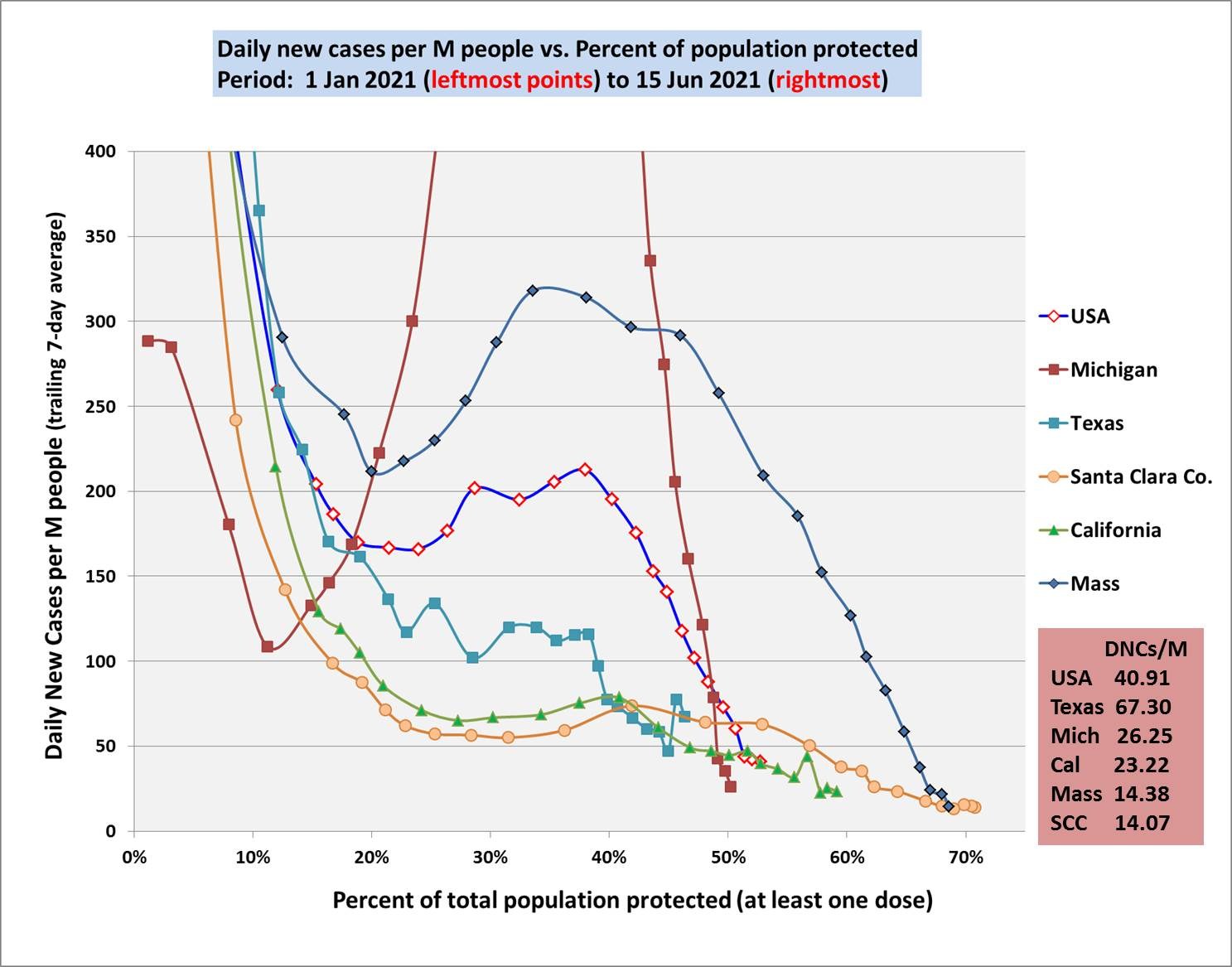
You can see how the case rate in the U.S. was eventually – in spite of our 4th wave of infections – driven down by the continued progress in vaccinations. The chart below shows the U.S., selected states, and Santa Clara County, CA. and the declining case rates as vaccinations increased and overcame the recent Spring surge in cases. (click to enlarge)
So we know – as with smallpox, measles, and Polio – that vaccines work to defeat diseases; it just takes decades.[7]. The CDC recently published age stratified data covering the period from Sept., 2020 up to May 1, 2021, so we can see the effect that vaccinations have had this past spring, at a national level. The data provides pretty clear evidence that the vaccines are working to reduce not only COVID cases, but COVID-related Emergency Department visits, hospitalizations and deaths – particularly among seniors.[1]
What is also encouraging is news that vaccines work BETTER than immunity acquired from getting sick with COVID and then recovering. Among three reasons for that improved defense is that natural infection only exposes the body to the virus in the respiratory tract (unless the illness is very severe), while the vaccine is delivered to muscle, where the immune system may have an even better chance of seeing it and responding vigorously.[2]
Further vaccine good news is that unlike the situation for the common cold, we have now developed multiple COVID-19 vaccines. The evidence continues to suggest that acquired immunity from vaccines still offers substantial protection against the new variants now circulating around the globe. There’s even another new vaccine from Novavax which is testing EVEN BETTER than Pfizer and Moderna, and is 90% effective against some variants. And the Novavax solution is cheaper and easier to manufacture, with less side effects. It hasn’t yet been produced in volume, and we now have more doses of U.S. vaccines than people willing to take them, but this new one should help the rest of the world, and reduce the chances of a ‘vaccine rebound’ returning to our shores.
Finally, CDC Director Walensky says that adult Covid deaths are now ‘entirely preventable,’ thanks to vaccines. With luck, we might have vaccines approved for children under Emergency Use Authorization by the fall.
The Bad
First, a well-run UK study now proves there is permanent loss of brain tissue in COVID survivors.[3] The brain areas affected are involved in smell/taste, cognitive function, and memory formation. And the unpleasant surprise? Most of COVID patients examined had had only mild to moderate disease in the past. Because they do Public Health better than we do,[6] the Brits have been following the health of over 500,000 people for years, including taking 40,000 initial brain images before the Pandemic. By comparing before and after brain images for those people who had COVID, with others of similar characteristics who did NOT, researchers found the loss of brain tissue. This study explains the cause of Long COVID symptoms documented in prior studies.
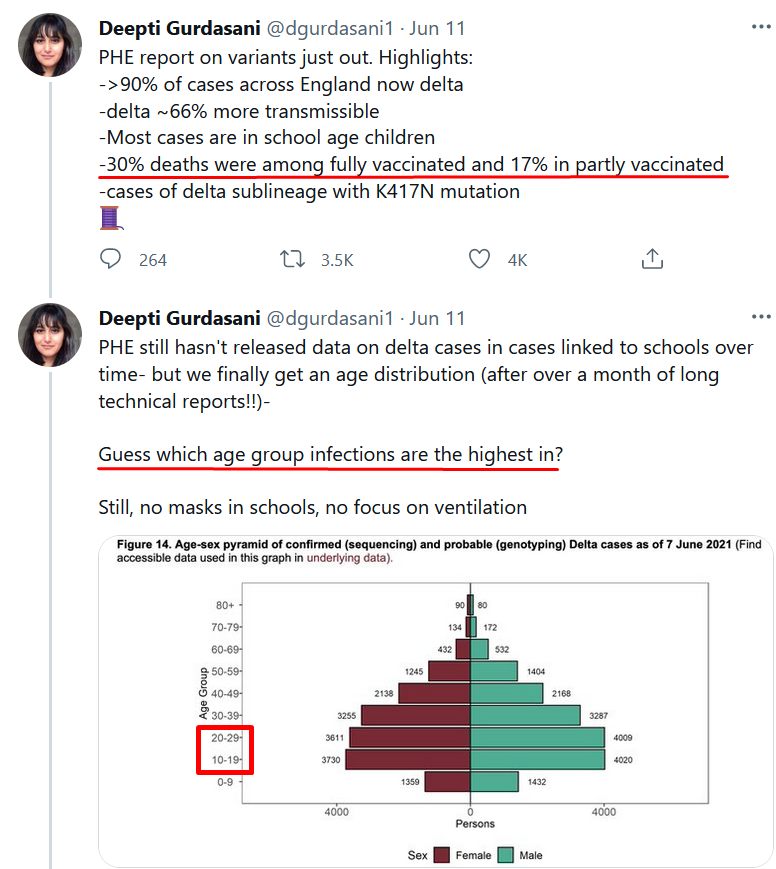
Then we have the OTHER UK bad news (at right->):
- Most cases are now school age children…
- 30% of deaths were fully vaccinated and 17% partially (UK is about 2/3rds AstraZeneca vaccinations)
- 90% of cases are the Delta variant
The Ugly
The virus doesn’t care whether you believe in vaccine science or not. It just wants to survive and grow.
The transmission of the more contagious Delta variant in the United States could spur a fall surge in coronavirus infections if only 75 percent of the country’s eligible population is vaccinated, former Food and Drug Administration chief Scott Gottlieb said Sunday. In fact, our hopes for herd immunity, which used to focus on a 70% level of population immunity, have been dashed. The new variants now put us in Measles Territory, where over 90% of the population has to be immunized to stop further cases from spreading.[4]
I wish we could end on a higher note, but the only way we’re going to put this Pandemic behind us is to gather the facts, and act on them. Get everyone you know vaccinated. And remember Dr. Michael Osterholm’s analogy:
When you get vaccinated, it’s like buying a fireproof suit that works 90 to 95 percent of the time, but it doesn’t work all the time. So why walk into a big fire if you don’t have to?”
And a late addition, speaking of Ugly, THIS… The really bad part is in the small print.
FOOTNOTES:
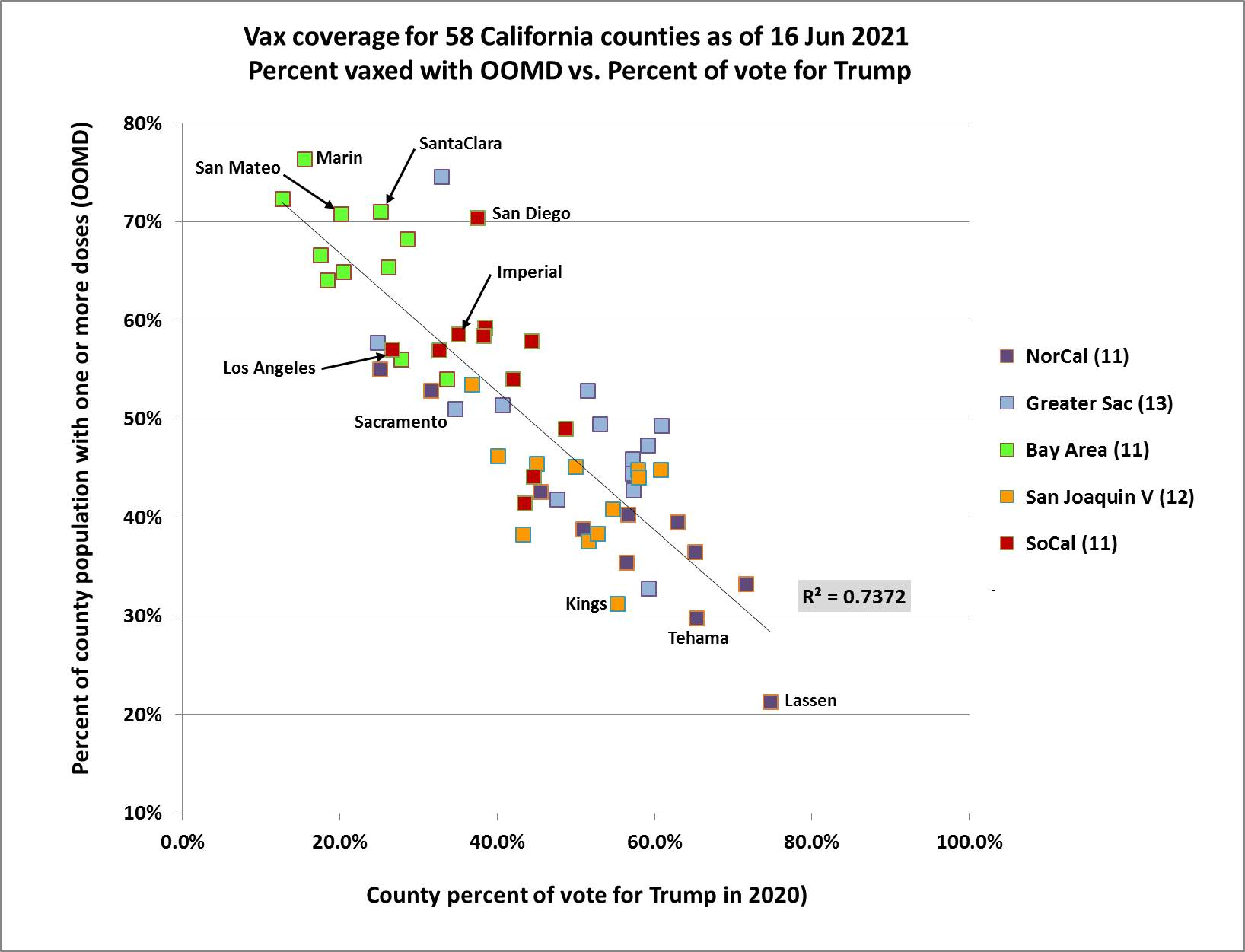
Pop Quiz Answer: Causes of Vax Resistance
Yep, at the same moment in time in this country we have both: 1) vaccines obviously providing resistance to the virus, and 2) resistance to the concept of Vaccination. As the data shows (chart right), it’s not either Cause A: fear of death and disability causing more vaccinations, or Cause C: being poor and lacking access to health care which prevents vaccination, which most strongly correlate with the rate of vaccination. It’s a Belief System tied to Trump that prevents people from being vaccinated. You would think that people living in an area where many of their neighbors got sick and died would be highly motivated to get vaxed. But no. There are other forces that determine vax rate.
[1] U.S. Vaccine Benefits
See: Athalia Christie, et al, “Decreases in COVID-19 Cases, Emergency Department Visits, Hospital Admissions, and Deaths Among Older Adults Following the Introduction of COVID-19 Vaccine — United States, September 6, 2020–May 1, 2021.” CDC MMWR, 11 Jun 2021.
The report includes four time series graphs, one each for weekly new cases, emergency department (ED) visits, hospital admissions, and deaths. Each graph shows curves for three age groups: 18-49, 50-64, and ≥65, plus a fourth curve that is the rate ratio between the seniors group and the youngest group. Cases peaked for all age groups in late Dec 2020; while hospitalizations and deaths peaked about 3 weeks later, in mid Jan 2021. As you would expect, rates for seniors in all four categories are significantly higher than for the two younger cohorts. However, with vaccination rates among seniors much higher than younger groups, the ratio of hospitalizations and deaths between seniors and others is narrowing.
[2] Why Vaccines are better
https://directorsblog.nih.gov/2021/06/22/how-immunity-generated-from-covid-19-vaccines-differs-from-an-infection/
The new evidence shows that protective antibodies generated in response to an mRNA vaccine will target a broader range of SARS-CoV-2 variants carrying “single letter” changes in a key portion of their spike protein compared to antibodies acquired from an infection. … antibodies acquired with the help of a vaccine may be more likely to target new SARS-CoV-2 variants potently, even when the variants carry new mutations in the RBD. …A third difference is that natural infection only exposes the body to the virus in the respiratory tract (unless the illness is very severe), while the vaccine is delivered to muscle, where the immune system may have an even better chance of seeing it and responding vigorously. … Whatever the underlying reasons turn out to be, it’s important to consider that humans are routinely infected and re-infected with other common coronaviruses, which are responsible for the common cold. It’s not at all unusual to catch a cold from seasonal coronaviruses year after year. That’s at least in part because those viruses tend to evolve to escape acquired immunity, much as SARS-CoV-2 is now in the process of doing.
[3] UK Public Health Study
The patients in this study were among over half a million adult volunteers in a public health initiative known as UK Biobank – an ongoing longitudinal study of the health of British citizens, which began recruiting long term participants from all over the UK, back in 2006. Since then, hundreds of thousands of participants have been providing Biobank with data on general health, annual physical exam results, periodic blood work, hospitalizations, and diagnoses. Less frequently, smaller subsets of thousands of participants are asked to undergo more detailed tests, including MRI brain scans. One purpose for collecting all this data, is to enable medical researchers to develop better tools for early prediction of health issues: as participants age and develop a range of health problems, their data from earlier years can be re-examined for early signs that could have indicated future disease conditions. See:
https://www.ukbiobank.ac.uk/enable-your-research/about-our-data
[4] Loss of Herd Immunity
Stanford epidemiology expert Julie Parsonnet warns that COVID-19 vaccine hesitancy has probably made herd immunity unattainable, which makes vaccination all the more important for personal health. https://med.stanford.edu/news/all-news/2021/05/Herd-immunity-illusive-vaccination-best-to-stave-off-COVID-19.html
We need to stop pushing herd immunity to the public,” Parsonnet said, as it may discourage some people from getting vaccinated in the mistaken belief that, if other people get vaccinated, they can just wait for herd immunity.
Diseases such as measles and smallpox have been nearly eradicated, or at least heavily tamped down, thanks to widespread and effective vaccination. It’s unlikely the United States has actually reached herd immunity for measles, as many children are now unvaccinated… But COVID-19 is not measles. Unlike measles, not all cases of COVID-19 are symptomatic, so sick individuals can’t all be isolated; the COVID-19 vaccine is not 100% effective, and it’s unknown how long it bestows protection; there are many variants of the virus; and the virus can infect animals. “It took 40 years to control measles; for COVID, it is likely to take a lot longer to control,” Parsonnet said.
The other important thing to remember is that herd immunity is not this ah-ha moment where suddenly there’s no more disease and we don’t have to worry about it anymore,” Parsonnet said. “It’s something that must be maintained, mostly through vaccinations, once transmission has slowed down.”
[5] Emerging Variants
We have lumped four CDC Variants of Interest into the category “Other VoI lineages,” because none are currently growing very significantly in Cal. Two of these have been prevalent in NY state, but have not caught on much on the west coast. At the end of May the collective prevalence of all four was 9.2%. Individual prevalences were:
| Name | Code | % cases | Origin |
|---|---|---|---|
| no WHO | B.1.526.1 | 5.3% | NY, Oct’20 |
| Iota | B.1.526 | 3.7% | NY, Nov’20 |
| Eta | B.1.525 | 0.1% | UK, Dec’20 |
| Zeta | P.2 | 0.1% | Brazil, fall, 2020 |
Also:
| Name | April ’21 % Cases | May ’21 % cases |
|---|---|---|
| Gamma | 8.8% | 10.1% |
| Delta | 1.8% | 4.8% (rapid growth) |
[6] Tracking Public Health
In contrast to the 14 yr old UK effort with half a million people enrolled, a new US All of Us sponsored by NIH is now using data available from participants for COVID research. June 2020. Analyses may help reveal the origins of entry, spread and impact of COVID-19 in the United States. …All of Us will test blood samples from 10,000 or more participants who joined the program most recently, starting with samples from March 2020 and working backward until positive tests are no longer found. The tests will show the prevalence of novel coronavirus exposure among All of Us participants, and help researchers assess varying rates across regions and communities.
[7] Prior Vaccine Victories
The global eradication of smallpox was certified, based on intense verification activities, by a commission of eminent scientists on 9 December 1979 and subsequently endorsed by the World Health Assembly on 8 May 1980.[10][112] …The cost of the eradication effort, from 1967 to 1979, was roughly $300 million US dollars. Roughly a third came from the developed world, which had largely eradicated smallpox decades earlier. The United States, the largest contributor to the program, has reportedly recouped that investment every 26 days since in money not spent on (a) vaccinations and (b) the costs of incidence.[114]
*Jurisdictions refer to any of the 50 states, New York City, and the District of Columbia.
From January 1 to December 31, 2019, 1,282* individual cases of measles were confirmed in 31 states. This is the greatest number of cases reported in the U.S. since 1992. The majority of cases were among people who were not vaccinated against measles. Measles is more likely to spread and cause outbreaks in U.S. communities where groups of people are unvaccinated.
Global measles and rubella https://www.cdc.gov/globalhealth/measles/about/index.html In 1980, before widespread global use of measles vaccine, an estimated 2.6 million measles deaths occurred worldwide. While much progress has been made, including more than 23.2 million measles-related deaths prevented through vaccination from 2000 – 2018, measles still claimed the lives of 140,000 people (mostly children) in 2018. In 2018, measles infected over 9 million people. The health consequences of measles and rubella infection can be lifelong, including economic losses for individuals, families and societies.
Global measles outbreaks https://www.cdc.gov/globalhealth/measles/data/global-measles-outbreaks.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fglobalhealth%2Fmeasles%2Fglobalmeaslesoutbreaks.htm COVID-19 is increasing the risk of measles outbreaks. Almost 41 countries have already put off, or may put off, their measles campaigns for 2020 or 2021 due to the COVID-19 pandemic. This increases the risk of bigger outbreaks around the world, including the United States.

More From Gregg Dieguez ~ “InPerspective”

Mr. Dieguez is a native San Franciscan, longtime San Mateo County resident, and semi-retired entrepreneur who causes occasional controversy on the Coastside. He is a member of the MCC, but his opinions here are his own, and not those of the Council. He lives in Montara. He loves a productive dialog in search of shared understanding.
<< Mr. Laird is another semi-successful, semi-retired MIT entrepreneur but with more degrees, living in Los Altos. They roomed and caused trouble together back in the day. Bruce produces a periodic newsletter on the science and implications of COVID-19. For a free subscription, contact Bruce at: laird2007@hotmail.com

